Therapeutic exercise
Prone T-Raise
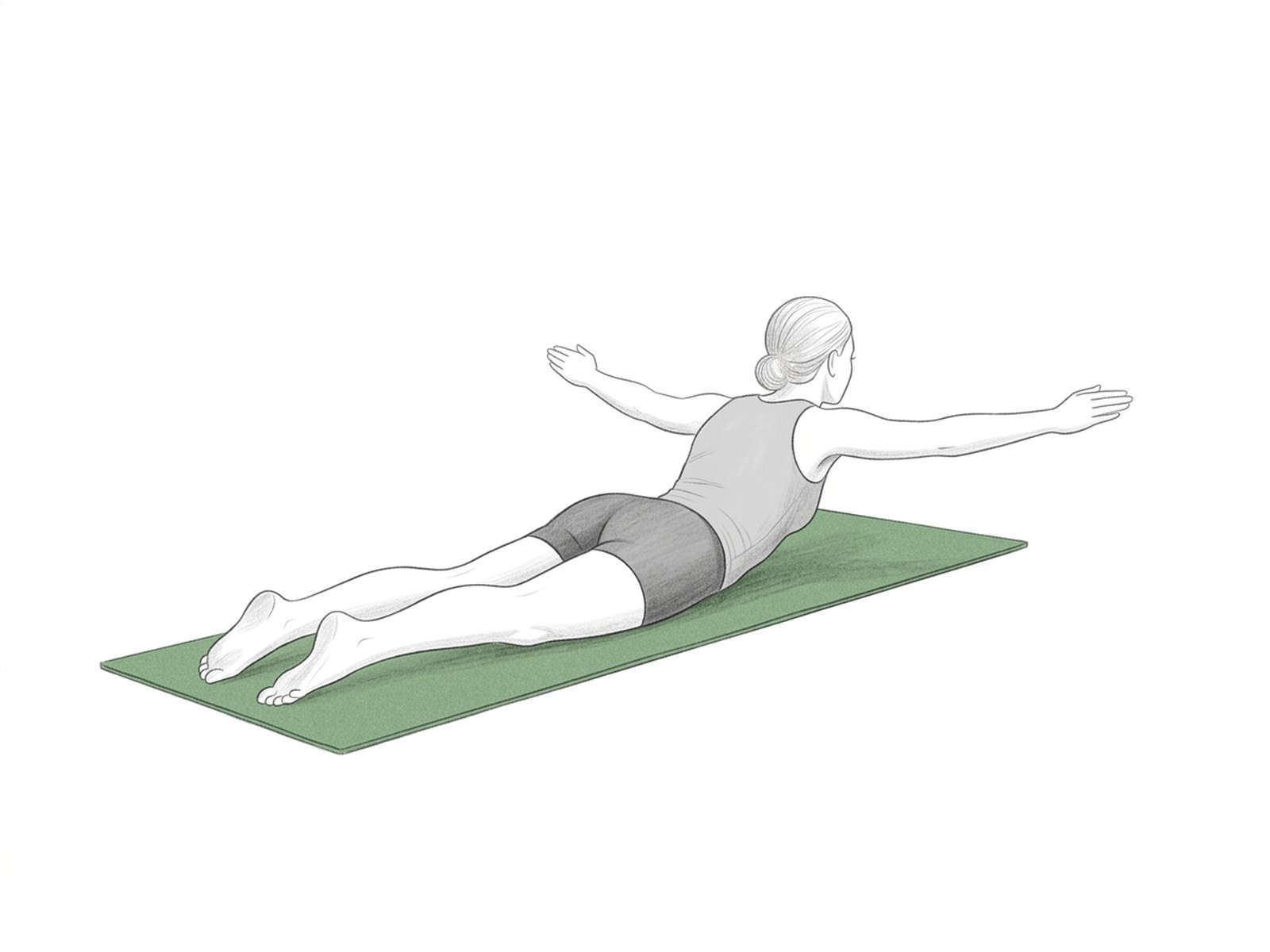
Isolation of the middle trapezius and posterior deltoid in a prone position. Component of the Prone I/T/Y/W series — essential for re-balancing the shoulder girdle in patients with upper-crossed syndrome and scapular dyskinesia.
How to perform
- Starting position. Lie face-down on a bench, with the chest supported and the arms hanging out to the sides, thumbs pointing up.
- Step 2. Open the arms laterally until they are aligned with the shoulders, forming a T with the body — elbows remain locked.
- Step 3. Squeeze the scapulae together at the top of the movement and hold for 2 seconds.
- Step 4. Lower the arms slowly over 3 seconds, resisting gravity.
- Return. Keep the neck aligned with the spine throughout the movement — look at the floor, not forward.
When not to perform
- Acute rotator-cuff injury
- Acute cervical pain in extension
- Recent shoulder surgery
- Glenohumeral instability
- Impingement syndrome in an acute inflammatory phase
- Thoracic pain in prone (costochondritis in acute phase)
Medical disclaimer. These exercises are presented for informational purposes only. Always consult your physician before starting any exercise program, especially in case of acute pain, recent injury, or underlying clinical condition.
Related Exercises
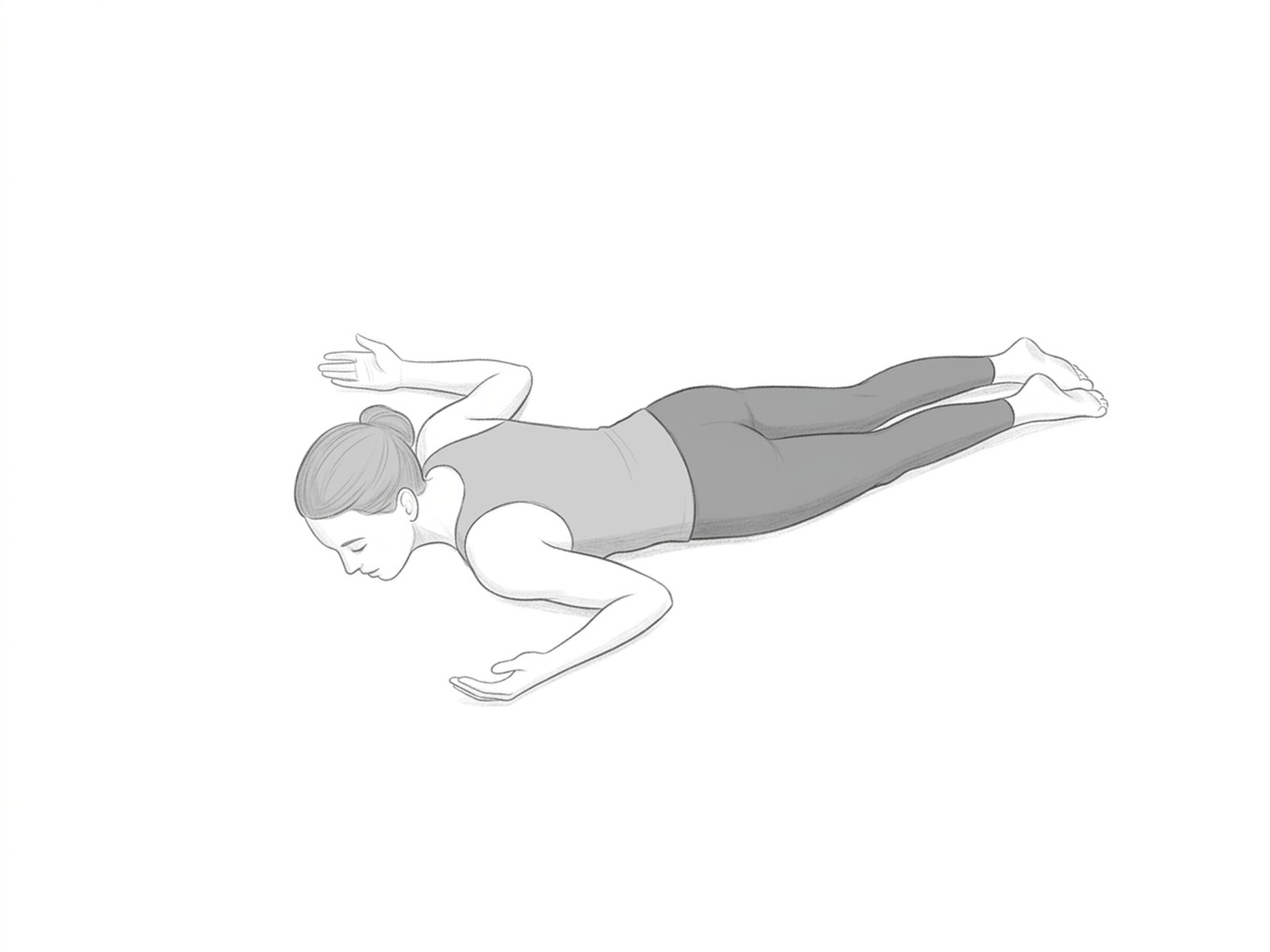
Prone W-Raise
Combines glenohumeral external rotation with scapular retraction in a prone position, forming a W with the body. Simultaneously recruits the posterior rotator cuff and scapular stabilizers — ideal for advanced progression of the Prone series.
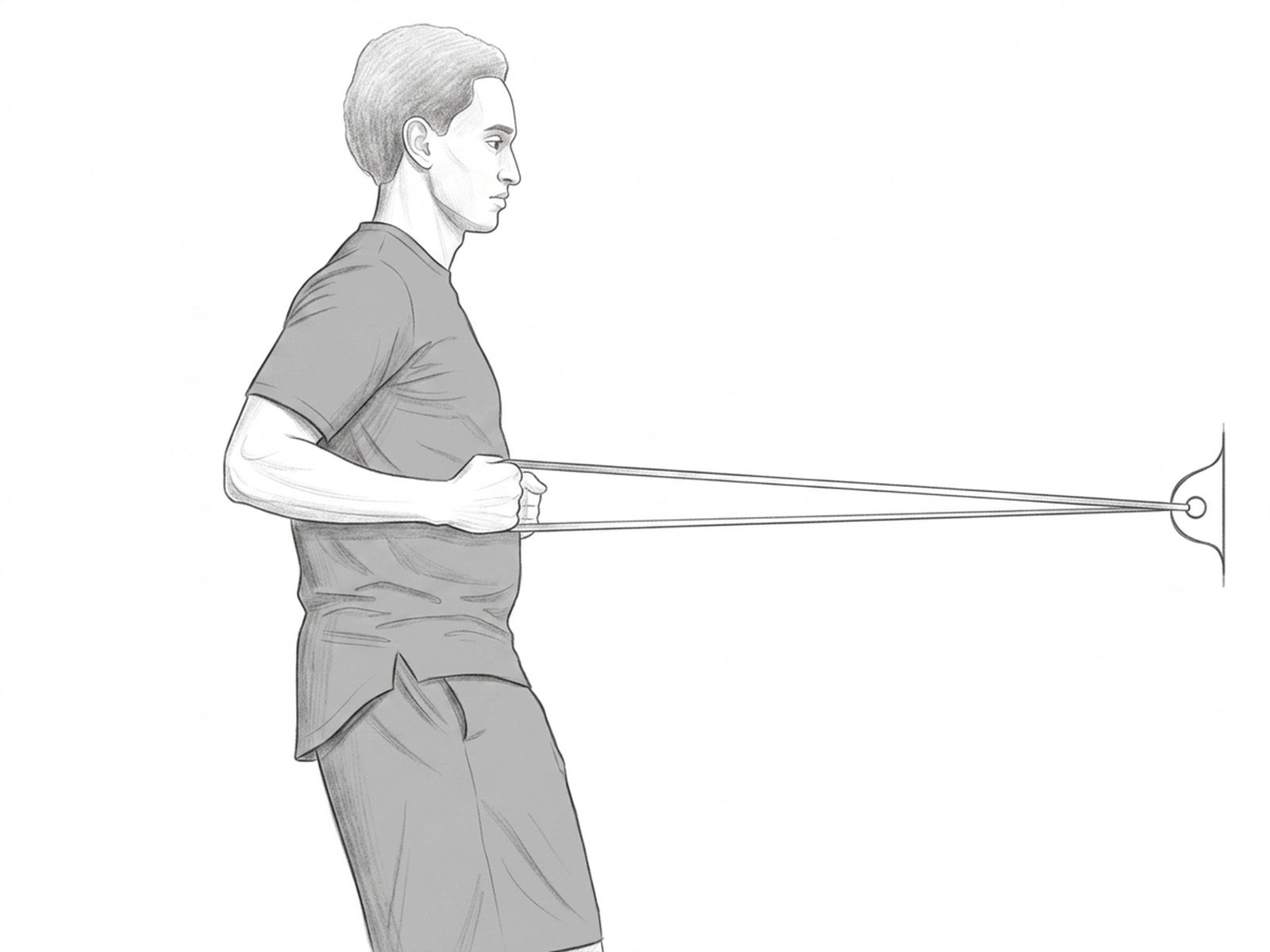
Banded Row
Horizontal pull with elastic resistance, recruiting the rhomboids, middle trapezius, and latissimus dorsi. The fundamental pulling exercise in shoulder-girdle rehabilitation — re-balances the pectoral/dorsal ratio in patients with upper-crossed syndrome.
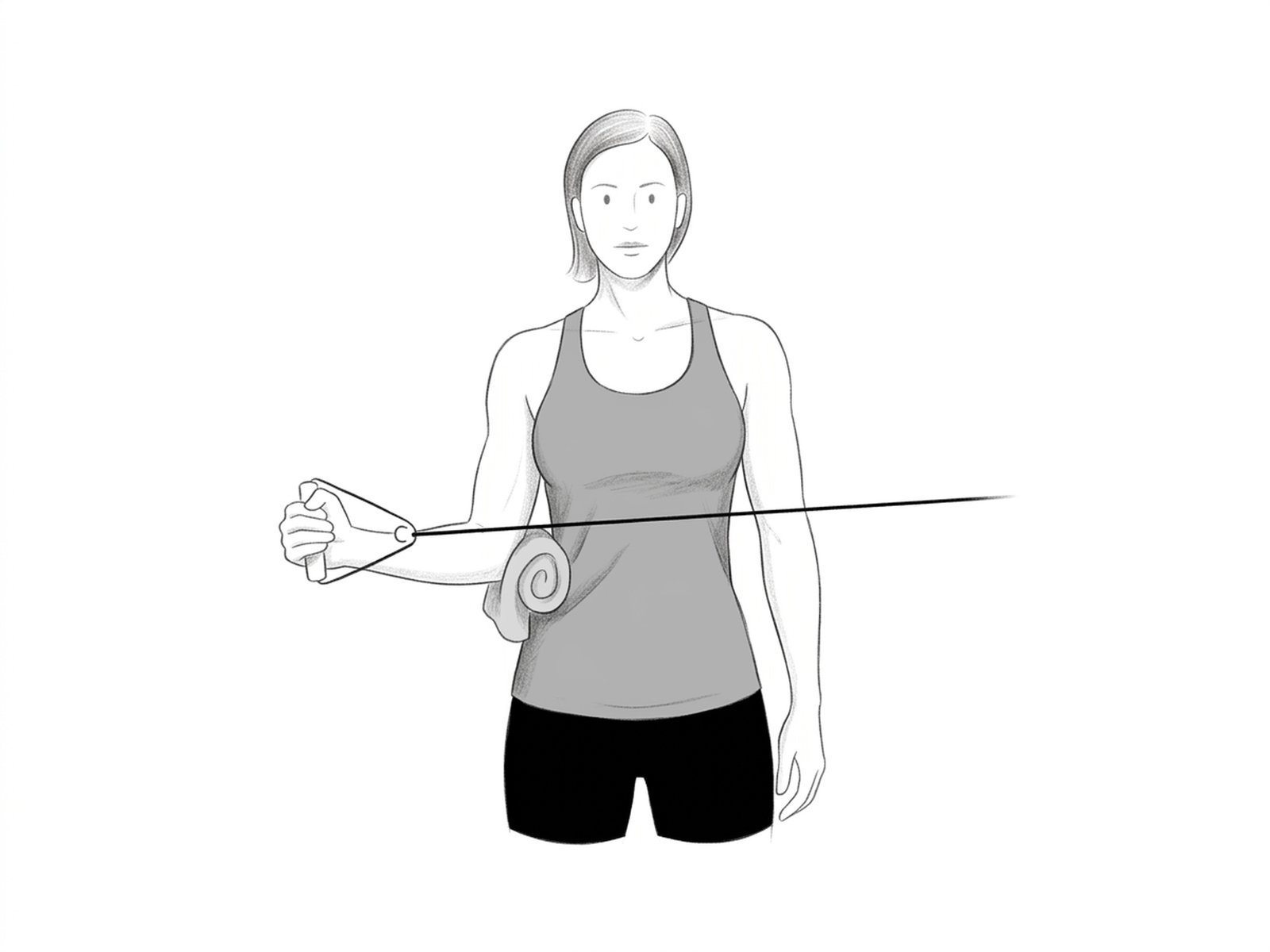
Standing Banded W
Standing version of the Prone W, performed with a resistance band. Simultaneously strengthens the external rotators and scapular retraction in a functional pattern that approaches daily activities — a progression from the Prone W when the patient already tolerates standing load.