Therapeutic exercise
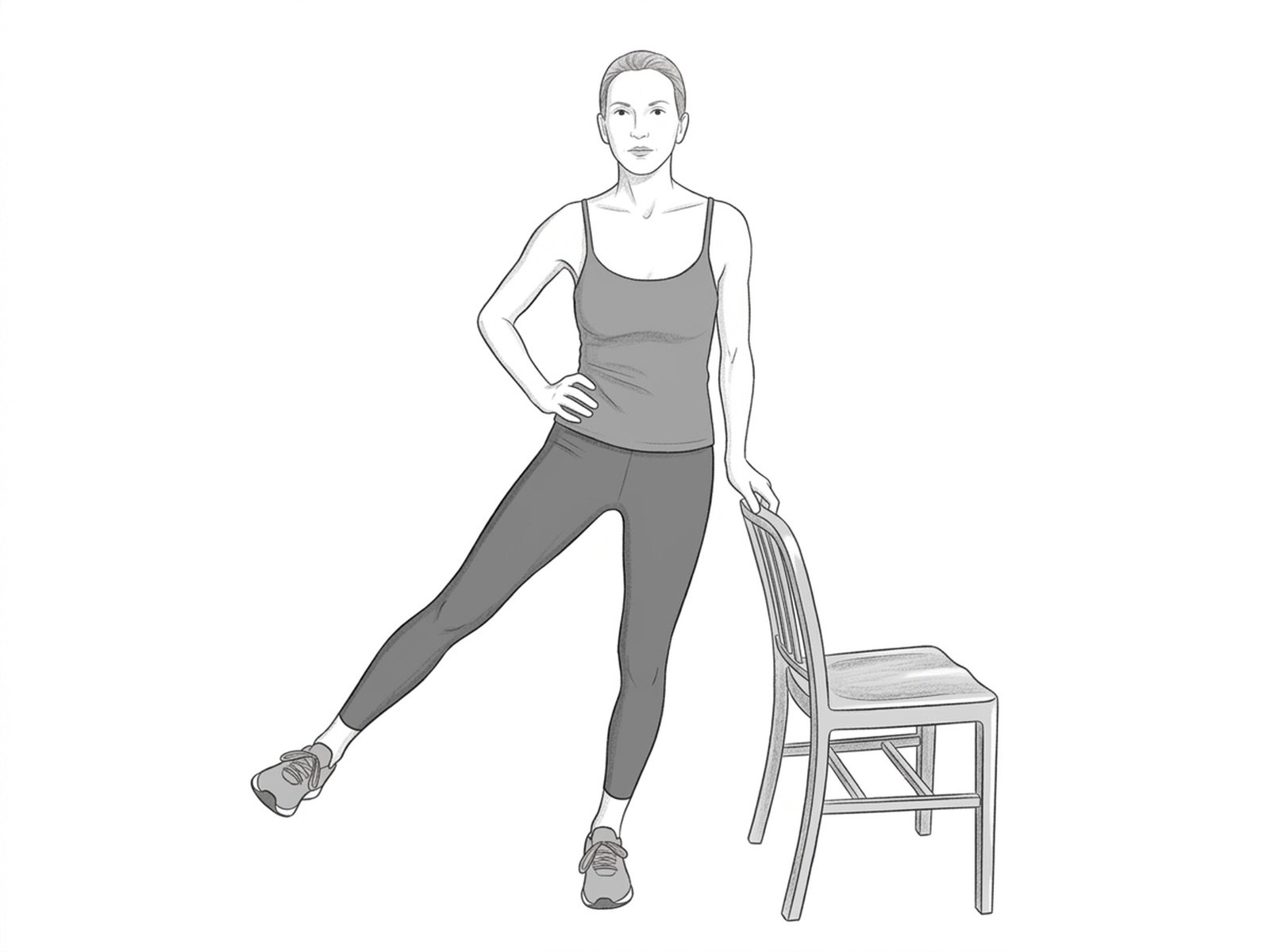
Standing Hip Abduction
Functional version of hip abduction performed in standing, in closed kinetic chain on the supporting side. Simultaneously recruits the abductors of the elevated leg and the pelvic stabilizers of the supporting side — closer to gait demands than the sidelying version.
How to perform
- Starting position. Stand beside a wall or chair for light support, with the feet hip-width apart.
- Step 2. Transfer the weight onto the support leg (the one farthest from the wall), keeping the trunk upright and the shoulders relaxed.
- Step 3. Slowly raise the free leg to the side (abduction), keeping the pelvis level — the movement comes from the hip, not from trunk lean.
- Step 4. Raise only to about 30 degrees — larger ranges tend to bring quadratus lumborum compensation.
- Return. Lower slowly over 3 seconds to the starting position and repeat. Complete a full set before switching legs.
When not to perform
- Acute hip pain or active trochanteric bursitis
- Ankle or knee instability without adequate support
- Recent post-operative hip surgery
- Femoral neck fracture in consolidation
- Positional vertigo
- Severe orthostatic hypotension
Medical disclaimer. These exercises are presented for informational purposes only. Always consult your physician before starting any exercise program, especially in case of acute pain, recent injury, or underlying clinical condition.
Related Exercises

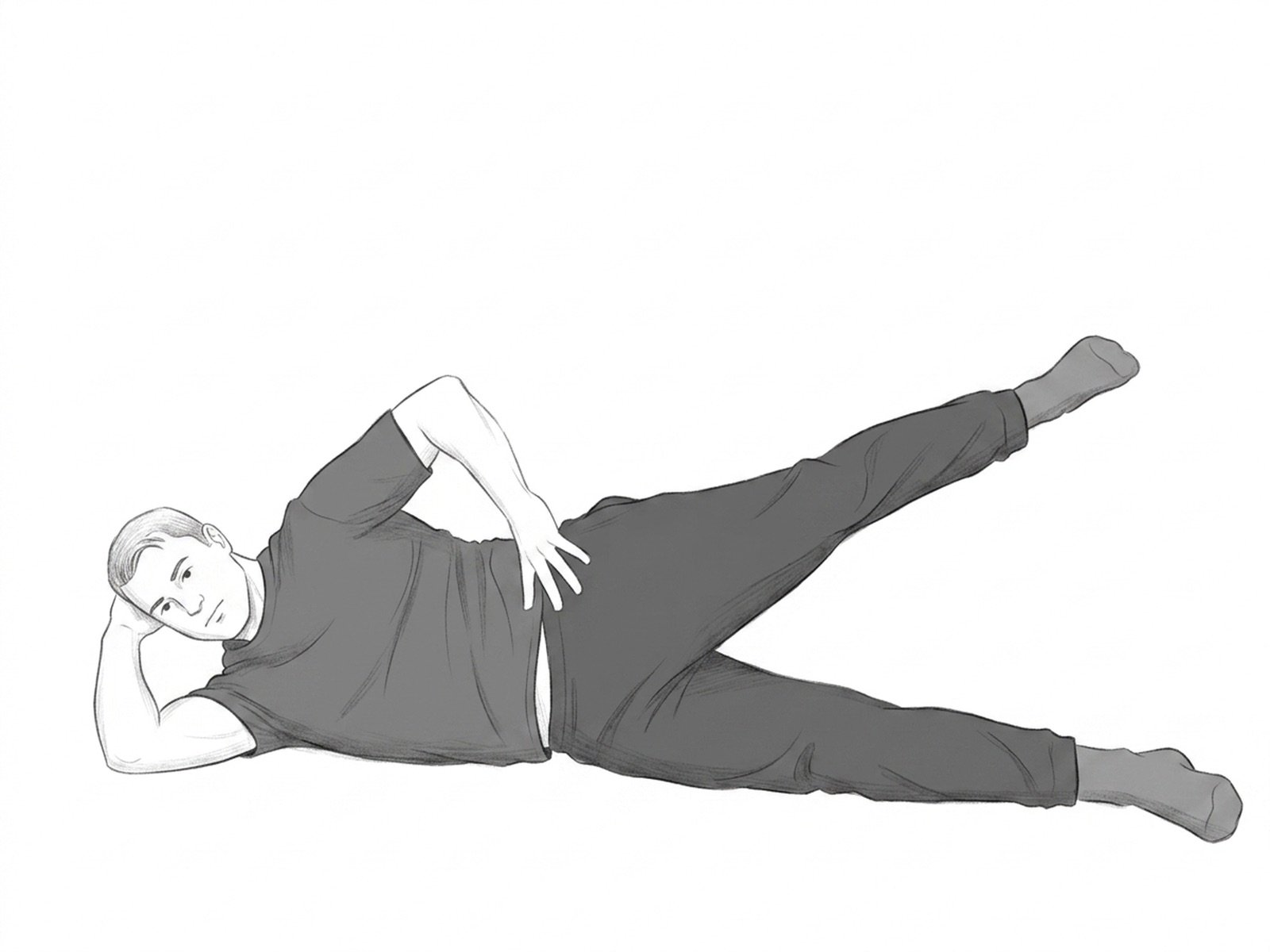
Side-Lying Hip Abduction
Strengthens the gluteus medius, a muscle frequently weakened in chronic sciatica. Improves pelvic stability during gait.
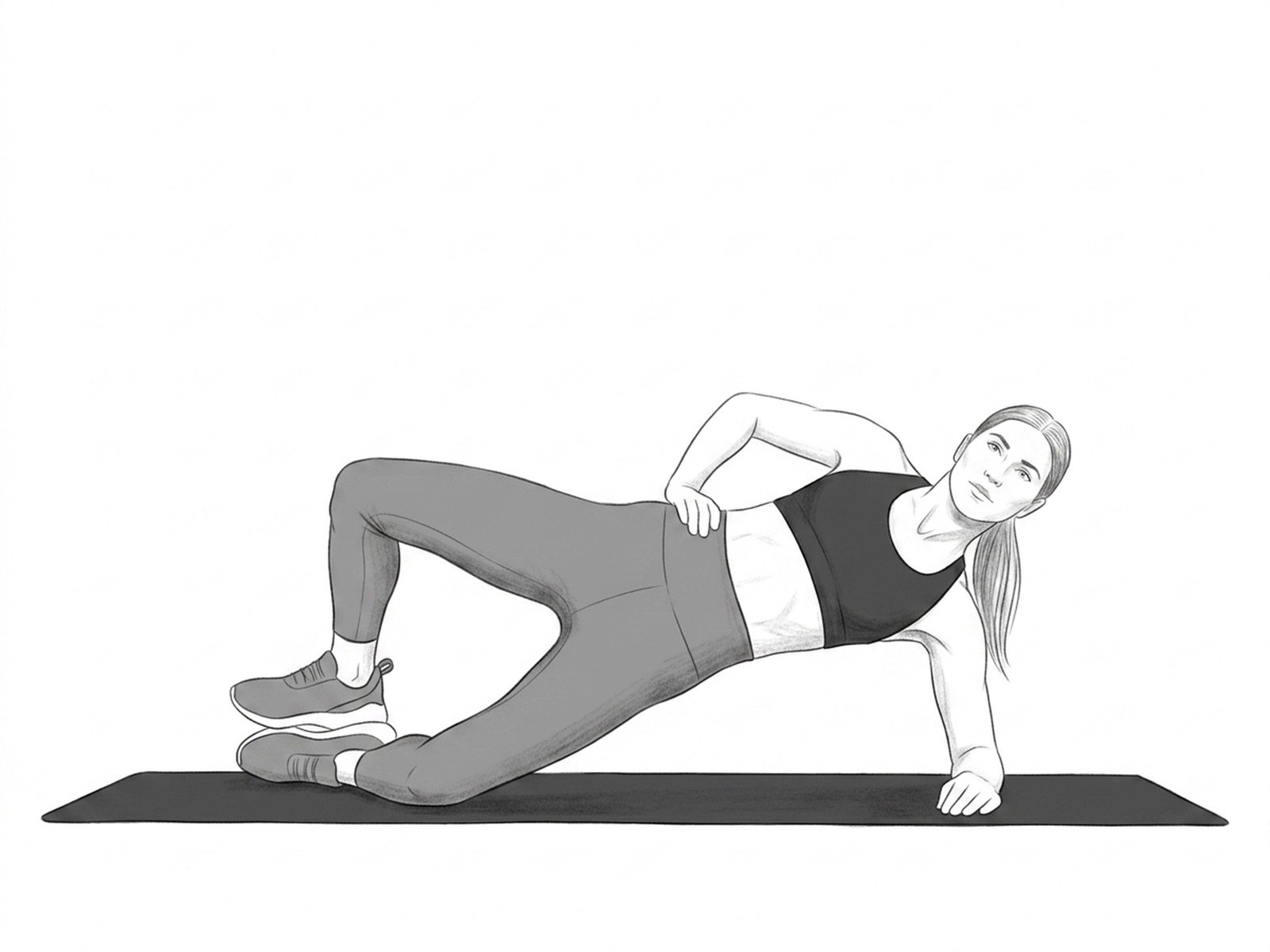
Sidelying Hip Abduction Isometric
Isometric version of the sidelying abduction exercise, holding the elevated leg without dynamic movement. In reactive gluteal tendinopathy, isometric loading produces an analgesic effect without overload — the first stage of treatment before isotonic work.
Clamshell
Strengthens the gluteus medius and the external hip rotators. Essential in hip osteoarthritis to reduce the compensatory Trendelenburg pattern during gait.