Therapeutic exercise
Sidelying Hip Abduction Isometric
Isometric version of the sidelying abduction exercise, holding the elevated leg without dynamic movement. In reactive gluteal tendinopathy, isometric loading produces an analgesic effect without overload — the first stage of treatment before isotonic work.
How to perform
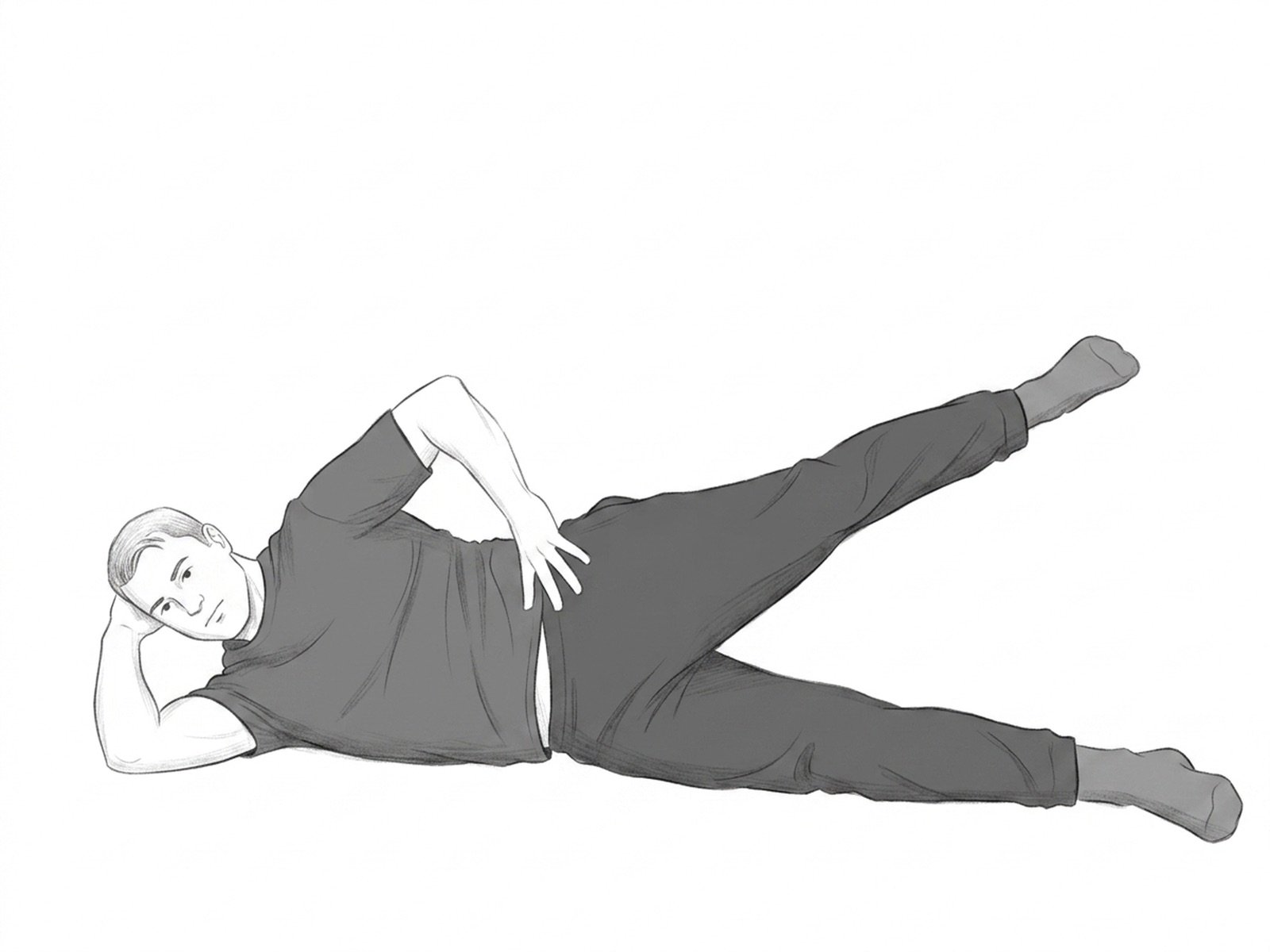
- Starting position. Lie on your side with the affected side facing up, body aligned, and head resting on the lower arm.
- Step 2. Slightly bend the lower leg to stabilize the body and keep the upper leg extended and aligned with the trunk.
- Step 3. Slowly raise the upper leg to approximately 30 degrees above the hip line — a moderate abduction position.
- Step 4. Hold the raised position for 30 to 45 seconds, with the foot neutral (toes pointing forward, not toward the ceiling).
- Return. Lower slowly and rest 1 minute. The key is sustained holding, not quick repetitions.
When not to perform
- Gluteal tendinopathy in a severe acute inflammatory phase
- Acute trochanteric bursitis
- Recent post-operative hip surgery
- Recent femoral neck fracture
- Uncontrolled arterial hypertension (isometric work raises blood pressure)
- Hemiparesis preventing adequate lateral stabilization
Medical disclaimer. These exercises are presented for informational purposes only. Always consult your physician before starting any exercise program, especially in case of acute pain, recent injury, or underlying clinical condition.
Related Exercises
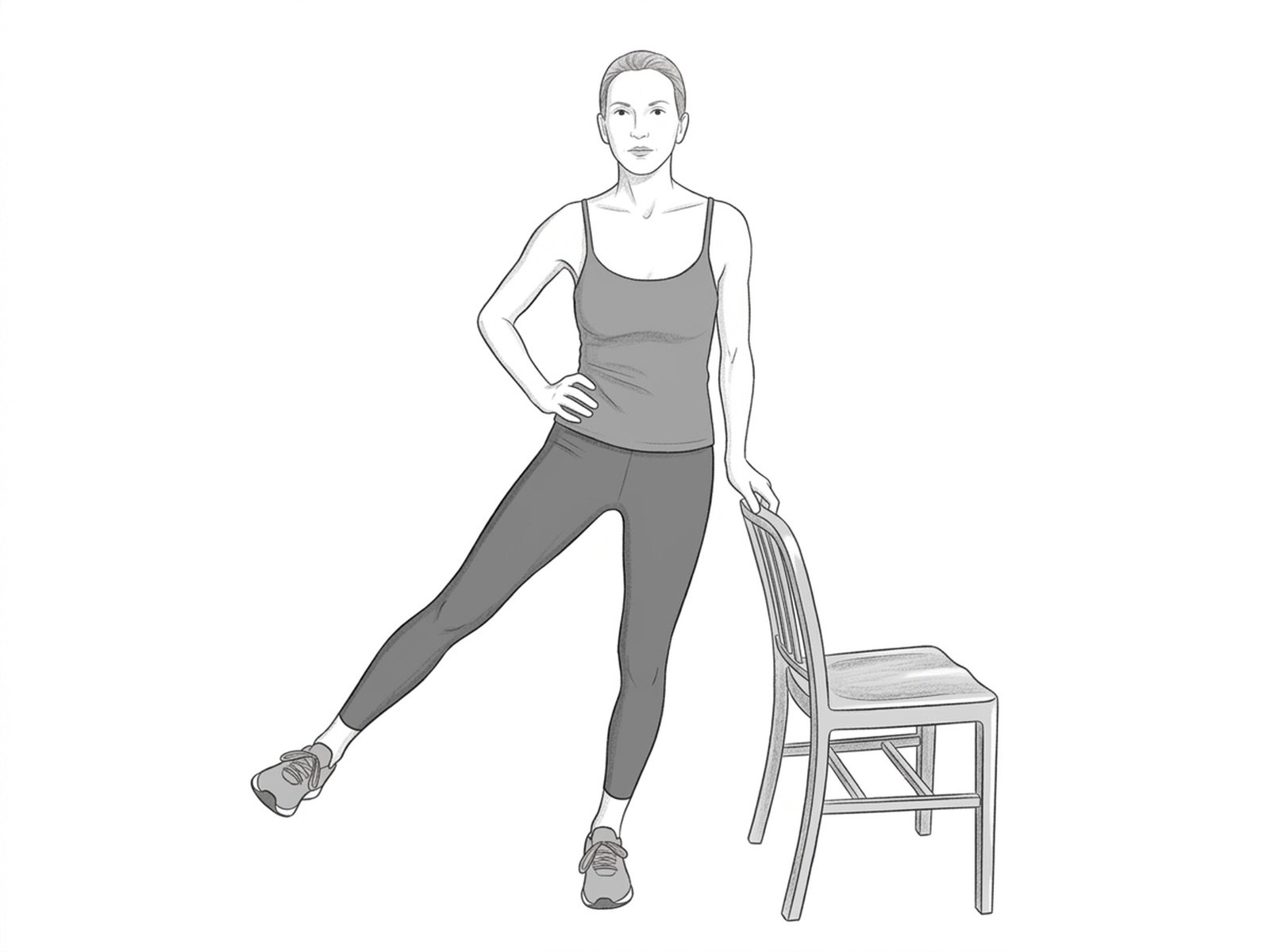
Standing Hip Abduction
Functional version of hip abduction performed in standing, in closed kinetic chain on the supporting side. Simultaneously recruits the abductors of the elevated leg and the pelvic stabilizers of the supporting side — closer to gait demands than the sidelying version.

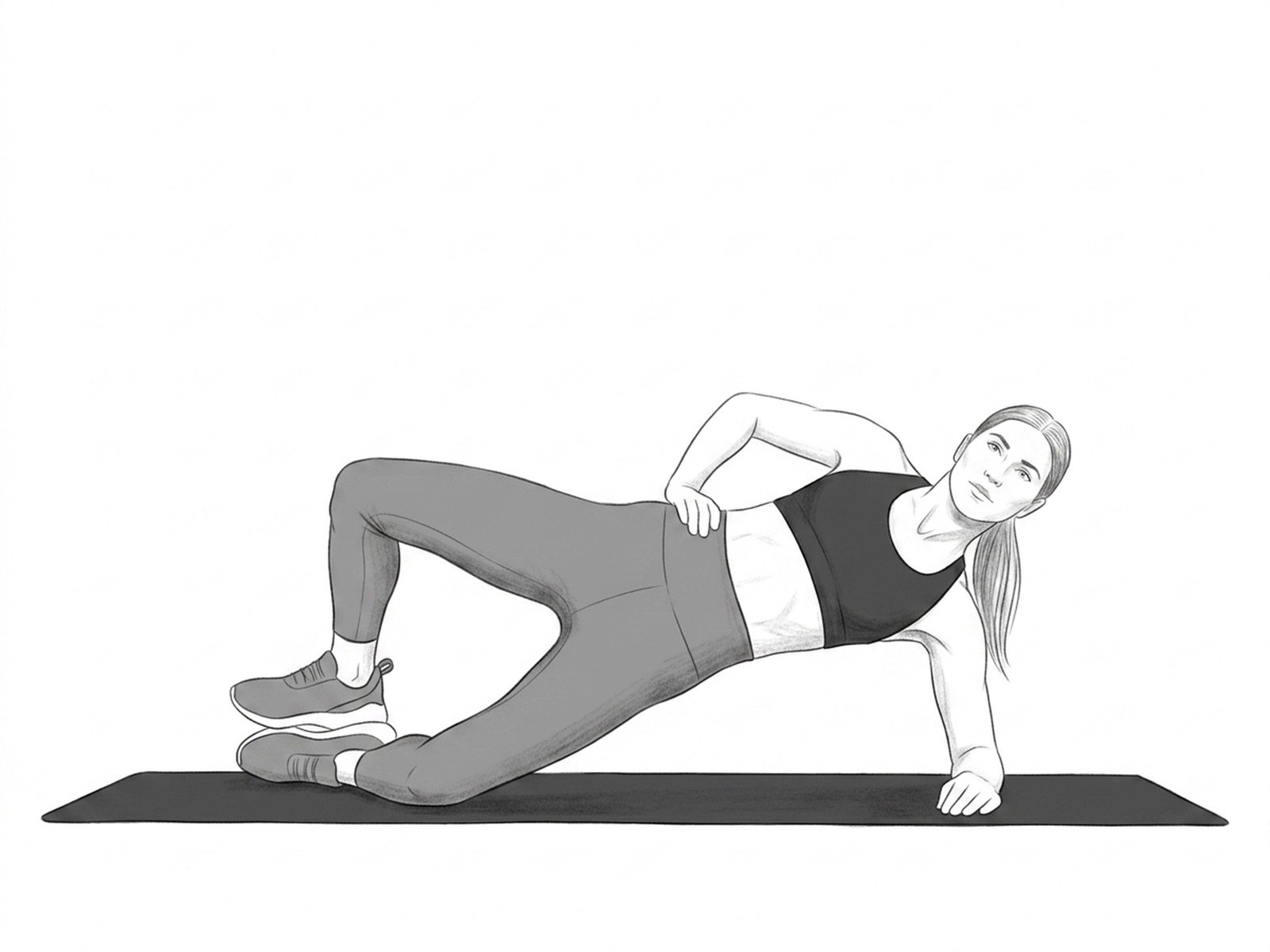
Side-Lying Hip Abduction
Strengthens the gluteus medius, a muscle frequently weakened in chronic sciatica. Improves pelvic stability during gait.
Clamshell
Strengthens the gluteus medius and the external hip rotators. Essential in hip osteoarthritis to reduce the compensatory Trendelenburg pattern during gait.