Therapeutic exercise
Scalene Stretch
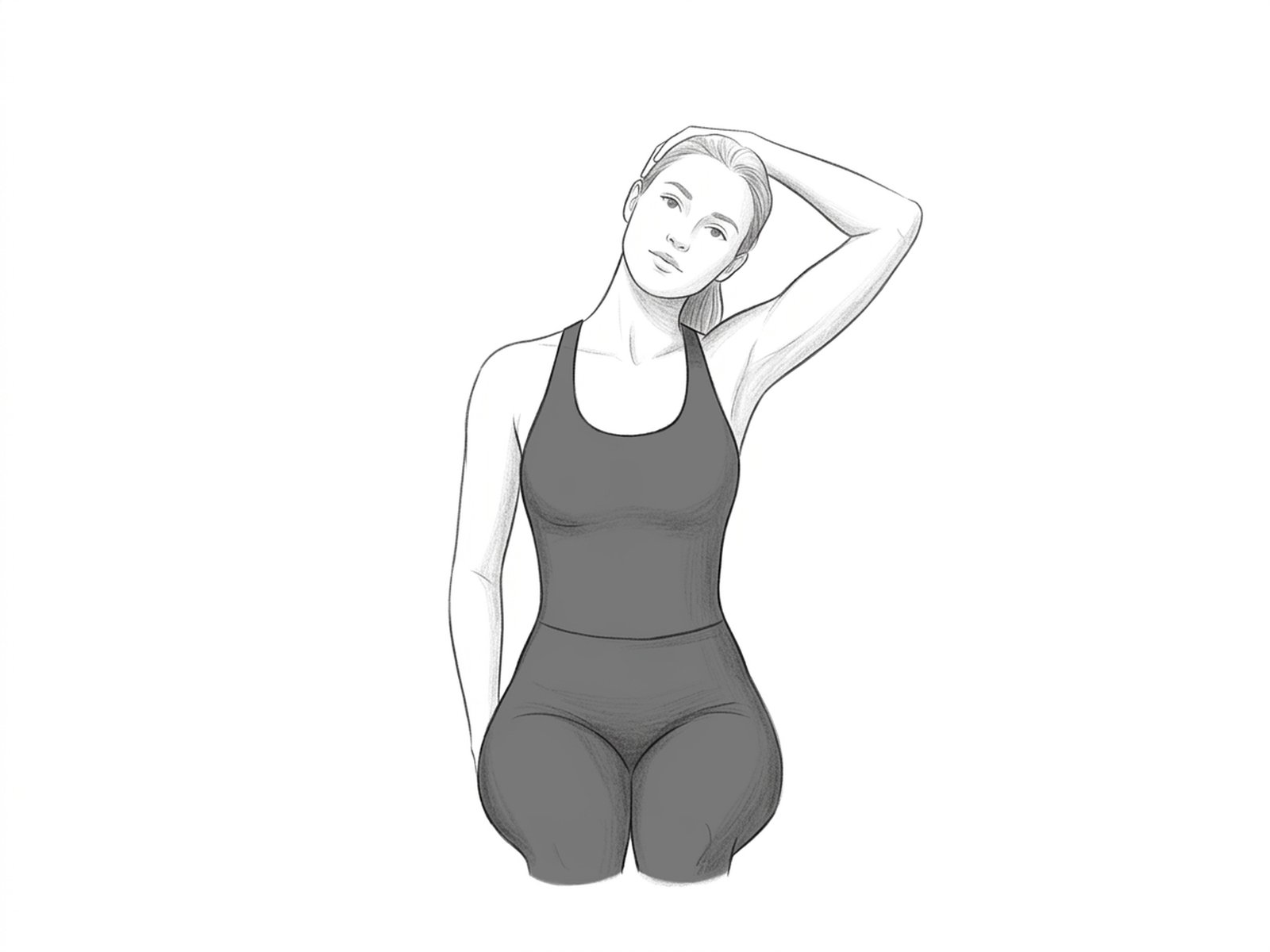
Specific stretch of the anterior, middle, and posterior scalenes — muscles that frequently compress the brachial plexus in thoracic outlet syndrome. Stretching them also helps mobilize the upper ribs, relieving cervical and high-thoracic pain.
How to perform
- Starting position. Sit upright in a chair, with shoulders relaxed.
- Step 2. Place the hand on the affected side behind the trunk and hold the chair seat or the lower part of the back — this depresses the clavicle.
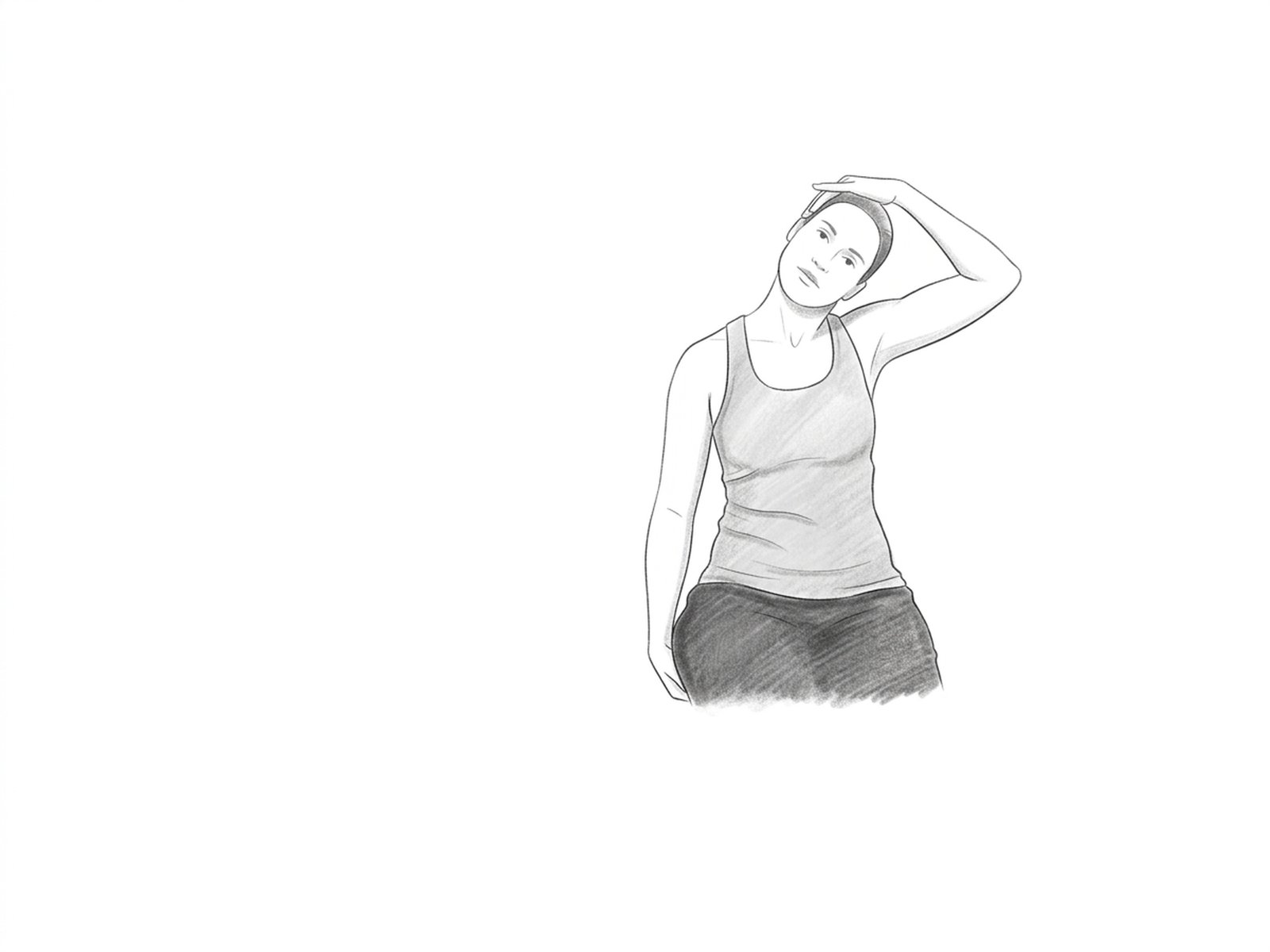
- Step 3. Keeping the clavicle depressed, tilt the head to the opposite side and slightly rotate the chin upward (toward the contralateral ceiling).
- Step 4. Feel the deep stretch on the side of the neck and upper chest region.
- Return. Hold for 30 seconds, breathing deeply. To reach different scalene fibers, vary the chin rotation: upward (anterior), neutral (middle), downward (posterior).
When not to perform
- Thoracic outlet syndrome in an acute neurological phase
- Vertebrobasilar insufficiency
- Cervical ligamentous instability
- Acute cervical radiculopathy with motor deficit
- Recent cervical trauma
- Acute cervical pain that worsens with the position
Medical disclaimer. These exercises are presented for informational purposes only. Always consult your physician before starting any exercise program, especially in case of acute pain, recent injury, or underlying clinical condition.
Related Exercises
Upper-Trapezius Stretch
Stretches the upper trapezius — a muscle that is commonly hypertonic in patients with mechanical neck pain. Relieves the sensation of heaviness and tension in the neck and shoulders.
Cervical Retraction (Chin Tuck)
Activates the deep cervical flexors — longus colli and longus capitis — muscles essential for cervical stabilization and frequently inhibited in chronic neck-pain patterns.
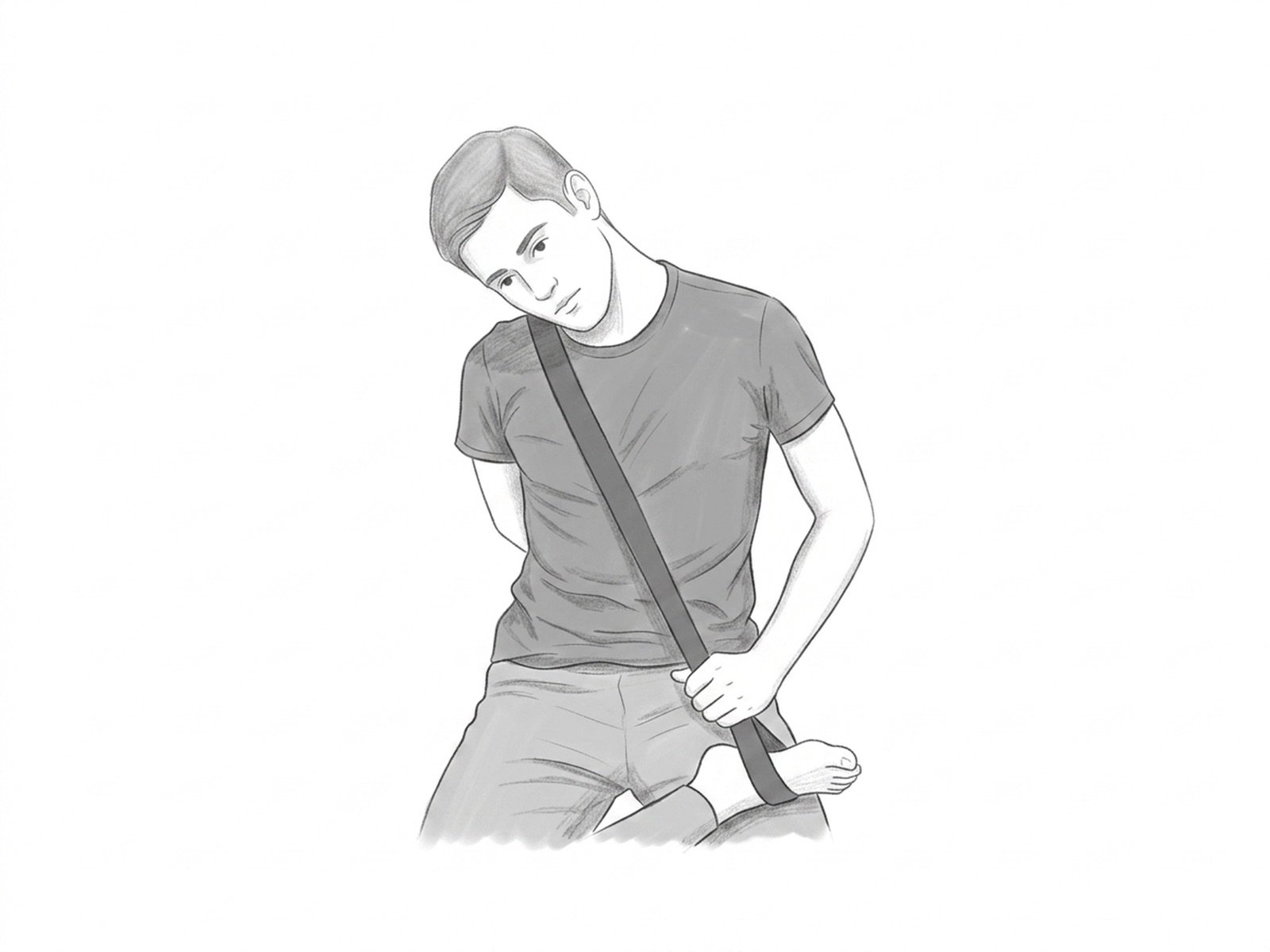
Self-Mobilization of the First Rib with a Strap
Self-mobilization technique for the first rib using a strap passed over it. Indicated in thoracic outlet syndrome, where elevation of the first rib contributes to neurovascular compression — descending mobilization relieves the syndrome.